
CKD is becoming more and more common…as is acceptance of patients to receive renal replacement therapy (RRT). The three types of RRT are Haemodialysis, Peritoneal Dialysis (PD) and Renal Transplantation. Peritoneal Dialysis can seem to be a bit daunting as it’s not as commonly seen outside of renal units, however these patients will get ill just like anyone else so you will come across them every so often in other specialties. Here we will provide you with some top tips to add to your renal toolkit to help you expertly mange them!
So….What actually is PD?
- PD is performed at home so is associated (generally) with a lot more freedom than if you have haemodialysis. Most patients will choose their dialysis option and PD is often chosen for this reason and most end stage renal failure patients are eligible to have PD
- The main contraindication to having PD is when a patient has had complicated abdominal surgery (abdominal hernias need to be corrected before PD can begin too)
- As long as you have the manual dexterity and cognition to be able to perform PD then you can have it (if not…sometimes you can get a carer or family member trained to do this)…as attaching the machine to your PD catheter can be fiddly and the bags heavy
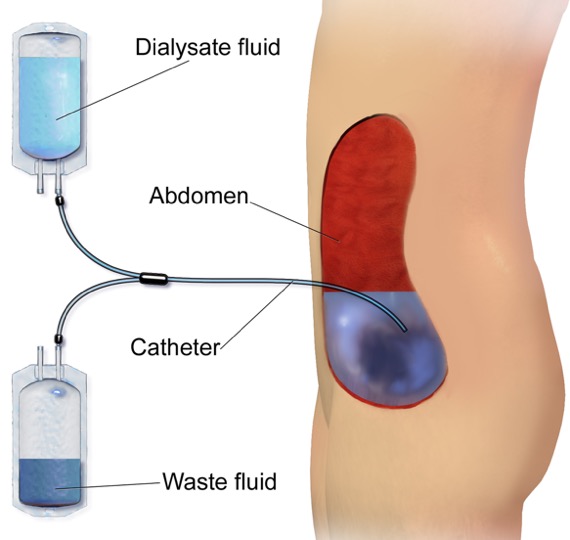
- PD uses the abdominal peritoneum as a membrane through which fluid, electrolytes and toxins from the blood are filtered and exit the body via a dialysate (a hypertonic solution) that sits in the abdomen and is then drained out [1]
- The dialysate fluid enters and is drained from the abdomen via a PD catheter…typically – a Tenckhoff catheter…
- A Tenckhoff catheter has an intra-abdominal portion (with holes in positioned in the pelvis) and an extra-abdominal segment (which exits lateral to the midline of the abdomen)
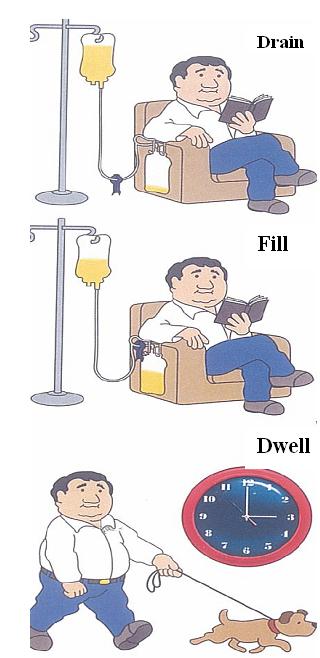
- There are two types of PD (based on patient choice/lifestyle preference)…
- CAPD (continuous ambulatory PD) – involves several manual exchanges during the day (done yourself) and usually a long ‘dwell’ overnight
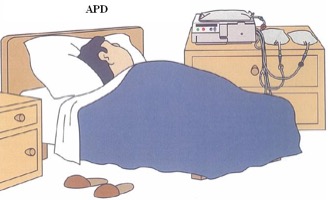
- APD (automated PD) – involves a long ‘dwell’ during the day and multiple cycles overnight performed by a machine by your bed whilst you sleep
- The patient (or carer) is trained in aseptic non-touch technique and will aseptically connect and disconnect their PD catheter from the APD machine or CAPD bags
- Like haemodialysis, PD does not completely takeover all the clearance of waste products and actions that a normal healthy kidney would, so…..
- Patients still usually need erythropoietin (as it’s no longer produced by the kidneys)
- Patients still get renal bone disease (as vitamin D metabolism and parathyroid hormone control stops working when the kidneys fail)
- Patients are usually on dietary fluid, phosphate and K+ restrictions
- Patients are prone to the same complications as HD patients such as infections and cardiovascular disease
- The PD patient will have a raised urea and creatinine BUT, if PD is working, then we should see a normal serum K+ and bicarbonate and the urea + creatinine should not be much higher than their usual trend
General Principles for the Unwell PD Patient…
- The MOST important point here is…to let the renal team/PD nurses know that the patient is in hospital…because:
- The patient may be too unwell to be able to perform their own PD or not have their equipment with them
- If there is no PD equipment in the hospital then they are likely to need to be transferred to their local hospital which has the equipment and nurses to provide PD
- PD patients often need adjustments to their PD script when unwell and the renal team/PD nurses can make/advise about these adjustments
- PD catheters should only be touched by PD trained nurses as the smallest contamination can result in PD peritonitis
- PD patients tend to get the same problems as HD patients…mainly infections and cardiovascular disease
- PD patients are often easier to manage than HD patients when they are unwell because:
- PD happens at home most nights so the patient is usually well dialysed i.e. less complications from underdialysis such as hyperkalaemia, uraemic complications etc.
- They are often quite compliant and involved in their own treatment as they usually have had to learn to dialyse themselves at home
- PD patients are more likely to have a better residual renal function than HD patients and those that do will have a better overall survival
- PD does not involve the more rapid haemodynamic shifts that a session on haemodialysis does
- If the patient attends your hospital feeling unwell…here a few ‘TOP TIPS’ to help with their general management whilst you treat the underlying cause of their illness….
- FLUID BALANCE:
- If the patient is on a fluid restriction – remember to maintain this in hospital
- They should also be on a salt-restricted diet
- Examine as you would for the usual signs of fluid overload
- Lying-standing or lying-sitting BP is a good measure of hypovolaemia (if BP drop >20/10 mmHg)
- Clarify how much urine the patient is passing – this will help you know if there is any RESIDUAL RENAL FUNCTION – if they are anuric then they will be much more prone to fluid overload and hyperkalaemia…
- Urine output is not a reliable marker of fluid balance or critical illness in these patients
- If dry/hypovolaemic: let the patient drink to thirst, cautious and small 250mls boluses of fluid with frequent reassessment is fine, contact the renal team or peritoneal dialysis nurses who will adjust their PD prescription appropriately so less fluid is removed by PD
- If euvolaemic: keep their usual fluid and dietary restrictions in place as normal and let the PD nurses/renal team know that they are in hospital anyway
- If wet/overloaded: If the patient still passes a reasonable (>0.5L/day) amount of urine (i.e. they still have some residual renal function) or if they are on diuretics normally then IV diuretics may help a little, make sure the patient is adherent to their fluid and salt restriction at home and in hospital, contact the renal team/PD nurses who will review their PD prescription…they may need to be given a more hypertonic dialysate to encourage more fluid removal
- If the patient needs it, then IV nitrates and CPAP can be given to help offload the patient of fluid but this is usually only a temporising measure and fluid removal is only likely to be achieved by dialysis
- DRUG PRESCRIBING:
- Many drugs (that are partially or fully renally cleared) can accumulate in PD patients (in the same way they do in HD or CKD) and some drugs are also dialysed so will need to be given at a certain time/levels monitored to ensure that the patient gets the correct dose
- Firstly…with any new drug you wish to give the patient – look it up in the renal drug handbook/database or check it with your clinical pharmacist
- Assume when you look up these drugs that the PD (or HD) patient has an eGFR <10
- When considering nephrotoxic drugs (such as Gentamicin)…try to consider alternatives (if possible) as although they are on dialysis, we want to preserve their residual renal functionas much as possible as this improves overall survival of the patient
- Be very cautious with opiate analgesics in these patients as they can develop toxicity – if they do, then Naloxone can still be given as in non-renal patients…
- If opiate analgesics are really required then consider brands that are less likely to accumulate in renal patients such as oxycodone or hydromorphone or buprenorphine patches…. check with your clinical pharmacist
- PROCEDURES:
- PD fluid needs to be drained out of the abdomen prior to certain procedures e.g. any abdominal and pelvic procedures/operations, endoscopy, colonoscopy and cystoscopy (so let the renal team know of operation/procedure dates)
- Prophylactic antibiotics are required for PD patients for the same procedures mentioned above to reduce risk of PD peritonitis (consult your local renal team)
PD Related Problems
- PD NOT WORKING:
- Problems with the dialysis machine or of the draining in and out of fluid should be and usually is discussed and dealt with by the renal team…
- If a patient is admitted to your ward unwell, look for signs that dialysis is not working, in addition to your usual patient assessment:
- Fluid overload signs
- Patient reports that their PD machine is alarming a lot, not working or the fluid isn’t draining in or out well
- Patient has missed their PD for a particular reason
- The patient is draining much less fluid out of their abdomen then the amount that went in
- The patient or you have noticed a possible leak of PD fluid somewhere else i.e. pleural leak (looks like a pleural effusion), subcutaneous leak (oedema to abdominal subcutaneous tissue)
- Pain on draining in or out
- Biochemical signs e.g. hyperkalaemia, acidosis or that their renal function looks much worse than their usual serum urea and creatinine
- ABDOMINAL PAIN:
- Here is a summary of the usual PD causes of abdominal pain:
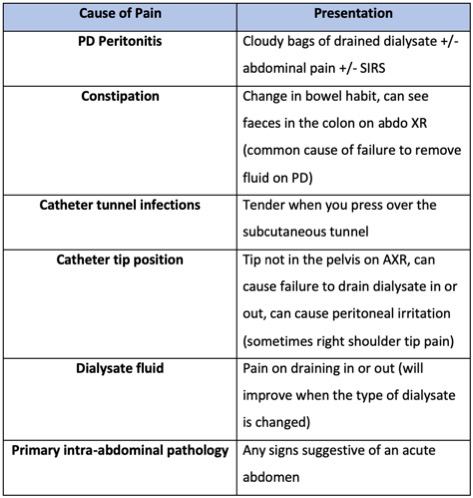
- Don’t forget the causes of abdominal pain you would consider in any patient i.e. gynae causes, pancreatitis, AAA, pregnancy, primary intra-abdominal pathology….so always check a lactate, amylase (and pregnancy test in women of childbearing age) and consider imaging such as CT
- PD PERITONITIS:
- PD peritonitis should be at the forefront of your mind when you see an unwell PD patient…however…they can look deceptively well despite this
- Recurrent or severe PD peritonitis can mean that the patient needs to switch to haemodialysis permanently
- So…how would we know if a PD patient has PD peritonitis? They can have any of the following in isolation or combination…
- Cloudy dialysate (fluid drained from the PD cavity)
- Abdominal pain
- Occasional systemic upset
- If this is suspected then the patient needs to have their dialysate sent for cell count and culture(the PD or renal nurses will do this for you)
- Diagnose if the dialysate cell count is >0.1×109/L with at least 50% polymorphonuclear leukocytes (neutrophils)
- Common gram positive organisms include coagulase negative staphylococcus or staphylococcus aureus (often from contaminated or infected PD catheter exit sites or tunnels) [5]
- Gram negative organisms are less common but multiple organisms (including anaerobes) can suggest a perforated viscus or something serious intra-abdominal. This will usually require more detailed imaging such as CT (and in some cases…surgical exploration) [5]
- Treatment is usually with intra-peritoneal antibiotics – these are put into the PD fluid that normally drains into the patient (by the PD nurses)
References
- Mehrotra, R. et al. The current state of Peritoneal Dialysis. JASN, 2016. 27(11): 3238-3252
- https://common.wikimedia.org/wiki/File:Blausen_0160_CAPD.png
- https://commons.wikimedia.org/wiki/File:CAPD.JPG
- https://commons.wikimedia.org/wiki/File:Illustration_of_APD_dialysis.jpg
- Bunke, C. M. et al. Outcomes of single organism peritonitis in peritoneal dialysis: Gram negatives versus gram positives in the Network 9 Peritonitis Study. Kid Int, 1997. 52(2): 524-529

{kind=link}
{kind=link}
{kind=link}